
The kidney transplant operation
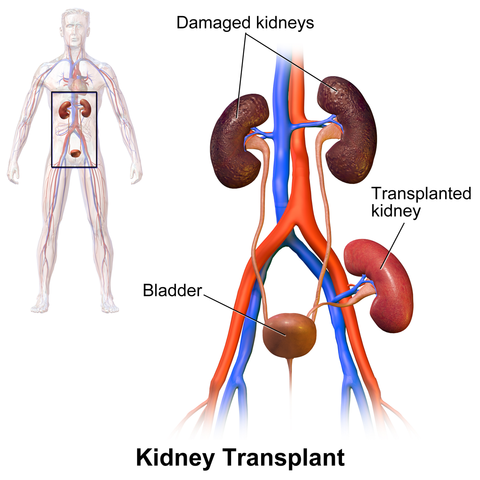
Kidneys are transplanted into the lower abdomen, close to the bladder and the large arteries and veins of the pelvis. This is done under full general anaesthesia (you are “asleep”). A curved or J-shaped incision (cut) is made, and the surgeon creates a space to place the kidney at the edge of the abdomen.
If the artery and vein are suitable for providing a blood supply to the new kidney, the surgeon joins the vein from the kidney to the big vein, then the artery from the kidney to the big artery. Once this is done, the kidney gets a blood supply and starts to recover.
The vein from the kidney is usually joined to the external iliac vein, which is the main vein taking blood from the leg and returning it to the bigger veins leading back to the heart. The artery is joined to one of the common iliac, external iliac or internal iliac arteries, depending on the length of the artery from the kidney and the condition of the iliac arteries. It is fairly common to have more than one artery from the kidney, and these can be joined together or joined to the iliac arteries in different places.
The surgeon then joins the ureter (urine pipe) from the kidney onto the bladder, or occasionally onto the ureter from the old kidney, so that the urine can flow into the bladder. To protect these joins, a plastic tube called a stent is placed in the ureter and passes into the bladder, and there is also a catheter in the bladder to drain urine to a bag outside the body. The catheter is usually removed after a few days, which is done at the bedside, and the stent is removed under local anaesthetic several weeks after the transplant.
A very small number of patients have problems with the bladder which make it unsuitable for passing urine after the transplant. If this is known before the transplant, we will make arrangements for a different way to drain urine, usually via a tube to the skin made from small bowel and known as an ileal conduit.
What happens after the operation
Patients usually wake up from the general anaesthetic in the recovery area of the operating theatres, then go up to the ward for postoperative care. You can expect to wake up with a catheter in the bladder, one or more cannulae (drips) in your veins and a central line (a tube going into a large vein in the neck or upper chest). You might also have one or more drains (tubes to remove fluid from deep in the wound) or local anaesthetic catheters (very fine tubes taking local anaesthetic to the wound to reduce pain).
The big incision (cut) needed to perform a transplant will be painful, so to reduce the pain you will get medication. This is usually a mixture of tablets and a system of giving intravenous doses of strong painkillers called a “PCA”: this has a button you press whenever you need a dose of painkiller. You might also have local anaesthetic in the wound, either injected by the surgeon or anaesthetist during the operation, or given continuously through a fine catheter passing through the skin.
PCA (“patient controlled analgesia”) is a system that gives a small dose of morphine or fentanyl whenever the patient presses the button. To prevent overdoses, it does not give a dose until at least five minutes after the last dose. It is very safe as the doses are small, but it is important to keep on top of the pain by pressing the button whenever sore. Only the patient should press the button - that is important for safety.
Local anaesthetic is given whenever possible, but not all wounds are suitable for giving it. When the wound is suitable for continuous infusion of local anaesthetic via catheters, that is our preferred option as we think it gives very good pain control.
We also usually give regular doses of paracetamol, which is actually a very effective painkiller when taken regularly after surgery and adds to the pain relief from other medications. Unfortunately we cannot give anti-inflammatory painkillers like ibuprofen as these can damage the new kidney.
The kidney might not work straightaway, so blood tests are done immediately after the operation to see if you will need dialysis to tide you over until the kidney starts to work.
Surgery tends to release potassium into the circulation, so it is common to need dialysis immediately after the operation. Dialysis will not harm the new kidney or make it take longer to recover. Patients who were getting peritoneal dialysis may need haemodialysis immediately after the operation as the peritoneum may have been damaged during the surgery - the anaesthetist will usually put a temporary dialysis line into a large vein in the neck to provide access for haemodialysis if the patient does not have access already such as a working fistula or graft; if such a line is needed, it is put in while you are asleep for the operation.

Once you are back on the ward, you will be able to eat and drink as soon as you have fully recovered from the anaesthetic as long as you are not nauseated or vomiting. If you have nausea or vomiting, the nurses can give you medication to make this better.
Post-operative nausea and vomiting is fairly common after a general anaesthetic. People who have had the symptoms after an anaesthetic previously are likely to get it again, and people prone to travel sickness are also more likely than average to get post-operative nausea and vomiting. Various medications can reduce the severity of the symptoms.
After abdominal surgery, the bowel does not always work well: this is called ileus. Ileus is uncommon after kidney transplant, but if it does happen you will be unable to eat until it has gone away; how long it takes to get better is variable, but usually loss of appetite happens with ileus, which makes the not eating a little more bearable.
We will aim to get you up and mobile as soon as possible. You will probably sit out in a chair later on the day of surgery and we will try to get you up and walking by the next day, or earlier if you are recovering well. Being up and about early will feel difficult, but is important as it improves lung function, reduces the risk of chest infections and blood clots and also improves bowel function.
We will arrange an ultrasound scan of the new kidney to check that it has a good blood supply. This is usually done on the first day after the operation, but is occasionally done on the same day.
If all goes well and the kidney starts to work, the nurses on the ward will support you in getting up and about, we will gradually reduce the pain control medication as the pain subsides and you will need to start learning the new medications you will be taking. There are renal pharmacists who come to the ward and can help with learning your medications. We usually take the bladder catheter out five days after the operation, although it may need to stay in longer if the bladder is small.
If the kidney is working well, you may be able to go home as early as six days after the operation, after which you will need regular attendances in the transplant clinic to keep an eye on how the kidney is working and to deal with any problems that come up.
What if the kidney does not work
It is common for the kidney to need a few days to recover. Losing its blood supply, being put in cold storage then being put into someone else is very unnatural and quite a shock to the kidney. While it is recovering, you may need dialysis, but this will not harm the kidney or slow down its recovery.
If after 5 to 7 days the kidney is still not working, or is not working well enough, we may need to get a biopsy of the kidney. This is a procedure done under local anaesthetic on the ward, and uses a needle to take a tiny piece of kidney and send it to the lab for analysis. The biopsy will tell us whether the kidney is just slow to recover or there is rejection.
Rejection happens in about a third of transplants and can usually be treated very effectively with additional anti-rejection medication. This is usually high dose steroids given as an intravenous injection, although in rarer cases of more severe rejection we also need to treat it with an infusion of antibodies called ATG. With modern anti-rejection drugs it is now very rare to lose a kidney from rejection in the early period of the transplant.

Complications of the Surgery
Most patients will get no complications or only very minor ones that do not need additional treatment, but there is a risk of more severe complications with any major operation. Most complications can be treated successfully, which may need additional medication or even further surgery.
Potential surgical complications include:
- infection, especially wound infections, chest infections and urine Infections
- bleeding, which may need a blood transfusion and/or further operations
- blood clots in the deep veins of the leg (DVT), which may spread to the chest and cause clots in the lung (pulmonary embolus); these are both fairly uncommon after kidney transplants
- wound complications such as minor or deep wound breakdowns
- fluid collections around the kidney; these are usually small and do not need treatment, but larger collections may need drainage by needle under local anaesthetic or even further surgery
- urine leaks, which might need the bladder catheter to be left in for longer; surgery is needed rarely
There are also complications associated with the immunosuppressant medication.
Recovery time
Most patients go home from the transplant ward around 6 to 10 days after the operation. How long you need to stay on the ward depends on how quickly the kidney starts to work, whether there is any rejection, whether you have any complications and how quickly you learn about and are confident with your new medications.
After leaving the ward, you will need to come to the acute transplant clinic at the Queen Elizabeth University Hospital regularly. For the first two weeks you will be seen twice a week, then the frequency of the appointments gradually reduces if all is going well. Around a third of transplant patients will need one or more readmissions to the ward if there are problems which cannot be managed in the clinic.
Patients generally need around three months before they are able to return to full time work, but the exact time taken varies from patient to patient and depends on how well the kidney is working, whether there are any ongoing problems and on the type of work done. Some employers will offer “phased return” which means returning to work part time and/or on light duties at first and gradually increasing hours and workload - this is often a good option if it is offered.
The kidney transplant diagram is by BruceBlaus and came from Wikimedia Commons.