
Haemodialysis access
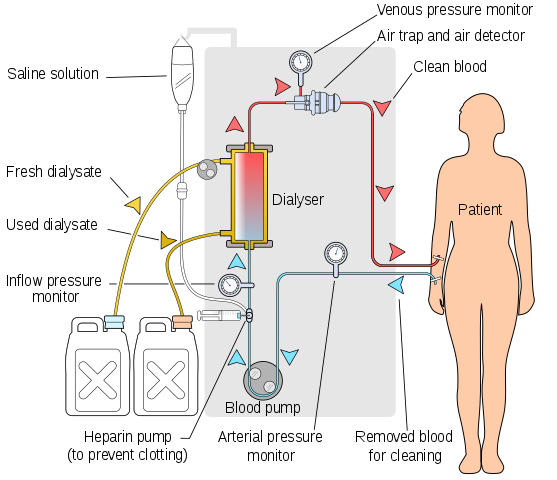
Haemodialysis sessions clean the body of waste products and toxins by a few hours of continuous flow of blood through a dialysis machine. Access to the bloodstream for haemodialysis is made by using a fistula, graft or line. These are explained below.
AV fistula
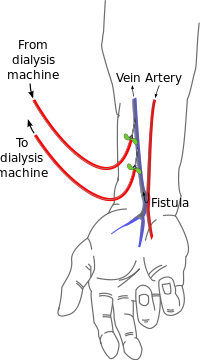
An arteriovenous (AV) fistula is a surgical join of a medium-sized vein to a medium-sized artery, usually in an arm, although it is also possible to make a fistula in the leg. The high pressure and flow from arterial blood makes the vein wall thicken so that it can be repeatedly needled for dialysis: this change in the vein is called maturation. Because it takes a few weeks to mature, it is best to make a fistula a few months before starting dialysis.
The ideal time to start planning dialysis access is around six months before the expected date of starting dialysis. This increases the chances of getting a good fistula working, and allows time for further procedures if necessary.
Fistulae in the arm can be made at the wrist, in the forearm or at the elbow. Generally we prefer to start as far along the arm as possible because if a fistula towards the end of the arm fails, it is possible to move further up the same arm to make a new fistula as the veins flow up the arm towards the heart.
The arteries and veins get smaller the further along the arm you get, so not everyone has a suitable artery and vein for a fistula at the wrist, and sometimes we need to start at the elbow.
Fistulae are the best form of access for dialysis as most patients with fistulae get more effective dialysis than patients with grafts or lines, and fistulae tend to get fewer complications and fewer hospital admissions. Whenever possible, we try to make fistulae for dialysis.
Veins can stretch, and so as the fistula is starting to mature the vein also tends to get wider and thus the rate of flow of blood through the vein increases. High rates of flow make dialysis more effective.
Not all patients are suitable for a fistula: if there are problems with the arteries or veins then it may not work. Sometimes problems are obvious and so we don’t even attempt a fistula, but at other times there is a chance the fistula may work so we do the operation. Even after the operation, the fistula can fail if it clots or does not mature.
The most common problem preventing a fistula is veins that have been scarred from blood sampling or drips. It is very important that patients with kidney disease avoid having needles put into these veins, especially in the veins of the non-dominant arm (e.g. the left arm if you are right handed). Please visit Save Your Vein for more about preventing this problem.
AV graft
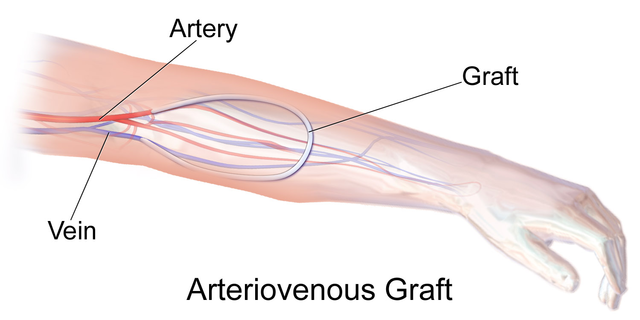
An arteriovenous graft is a plastic tube passing between an artery and a vein. It is a good alternative to a fistula for patients who do not have a suitable vein. The grafts we usually use are designed to be suitable for needling straightaway, so we also use them for patients who need to start dialysis urgently.
Grafts are usually placed in the arm but it is also possible to put them into the thigh, which is often the only option if there is narrowing of the veins in the neck and arms.
Some patients have customised trousers with a zip along the top of the trouser leg that allows the dialysis nurses to reach the graft without having to remove the trousers.
Grafts are nearly as good as fistulae in terms of effectiveness of dialysis, but if they become infected grafts often need to be surgically removed. If you have a graft, your dialysis nurse will be careful to use antiseptics and sterile gloves to minimise the risk of infection.
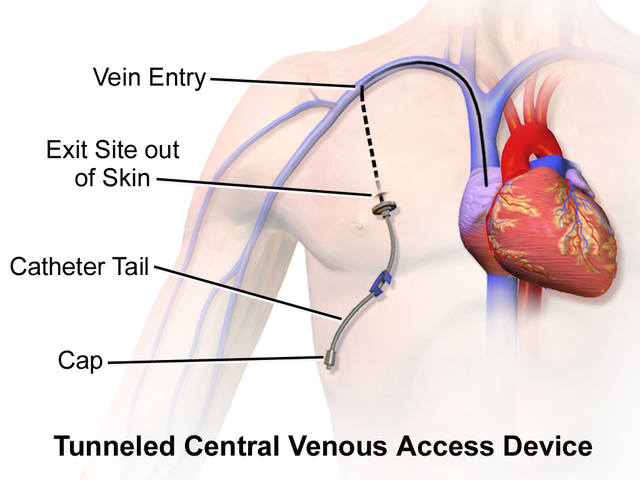
Dialysis lines
These are large plastic tubes going into a large vein in the neck or groin. Temporary lines go directly into the vein but can only be used for a few days. Lines for longer term use are tunnelled under the skin for a few inches then go into a vein; the tunnel under the skin is sealed by a cuff on the line, and this reduces the risk of infection.
Tunnelled dialysis lines should be seen as a last resort for dialysis access. They are prone to infection and blockage, and also tend to cause less effective dialysis than fistulae or grafts. In the longer term, they can cause permanent narrowing of the large veins of the neck and upper chest, which causes swelling of the face and arms and prevents further lines, fistulae or grafts being used in the arms or neck.
Dialysis lines have two channels, one to take blood out for filtering and another to return the cleaned blood, but the openings of these channels are only about an inch apart so there is some mixing of cleaned and unfiltered blood. The maximum flow rate through a line is also lower than that of a fistula or graft, and combined with the mixing effect this leads to less effective dialysis. If dialysis is less effective, you may need to spend a longer time on the machine at every dialysis session.
Because lines, like grafts, are made from plastic, bacteria can stick to them and thus infections cannot always be treated with antibiotics alone. If antibiotics do not clear the infection, then the line will need to be removed and new access for dialysis made; this will require a hospital admission of several days.
Fistulae and grafts have continuous flow of blood through them, but lines only flow while on dialysis. The lines are flushed at the end of dialysis to clear blood from the channels, but some blood may still get in and clot, blocking the line. We can usually treat this by putting clot-busting drugs into the line, but this does not always work completely and so the line may become narrowed which reduces the maximum flow and therefore the effectiveness of dialysis.
However, tunnelled lines do have their place. Patients who have no suitable arteries to provide blood flow for a fistula or graft will need lines, and tunnelled lines are a good option for patients who will only need short term dialysis, for example because they are about to get a transplant from a living donor.
The diagram of the dialysis circuit, radiocephalic fistula, AV graft and tunnelled central venous catheter are from Wikimedia Commons and by users YassineMrabet, Kbk, Blausen Medical and BruceBlaus respectively.